Our Take: Physicians Increasingly Employed by Health Systems
Mar 26, 2018

A new report from the Physicians Advocacy Institute and Avalere Health finds that 42 percent of physicians were employed by hospitals in 2016, compared with about 25 percent in 2012. There were 155,000 physicians employed by hospitals in 2016 and 95,000 in 2012—a 63 percent increase. And over the same time period, the number of physician practices owned by hospitals doubled.
Independent physicians are succumbing to the pressure of increased administrative costs because of increased reporting requirements stemming from the Affordable Care Act and other market forces.
“There’s the site-of-service differential, a multitude of regulations, stresses in dealing with electronic data,” Robert Seligson, president of the Physicians Advocacy Institute and CEO of the North Carolina Medical Society, told Modern Healthcare. “These are challenges for doctors and smaller practices.”
Our Take: Let’s stop for a minute and ask ourselves: is this trend such a bad thing?
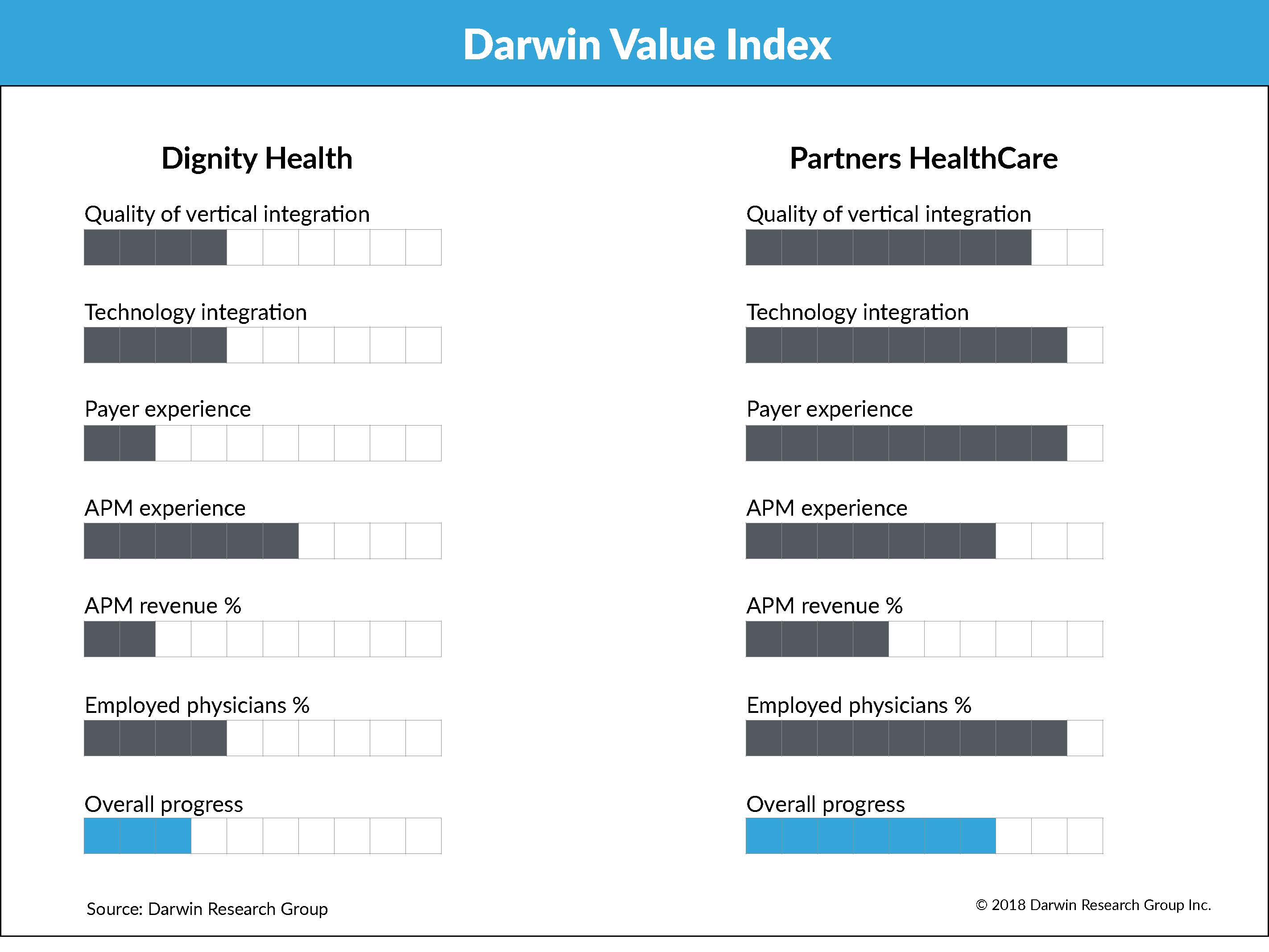
The Darwin Value Index (DVI) measures a health system’s progression from fee-for service to value-based care on a 10-point scale for six measures. While admittedly subjective, we determine these scores based on multiple interviews with health system executives. We update the DVI for about 100 health systems twice a year.
One of those measures is the percentage of physicians employed by the system. Why? Because we believe that systems have more control over physicians they employ, versus those who are affiliated with admitting privileges. Employed physicians are more likely to comply with, for example, a quality initiative that requires them to see a patient within seven days of discharge from a hospital stay.
If you agree that the U.S. is moving away from fee-for-service and toward quality, outcomes or value-based reimbursement, then it’s logical to conclude that hospitals would want to “own” their docs.
Now, some research suggests that health care costs go up when physician groups are owned by health systems. As recently as 2015, researchers concluded: “Financial integration between physicians and hospitals has been associated with higher commercial prices and spending for outpatient care.” In this study, there was a 3.1 percent increase in outpatient spending among integrated physician practices compared with independents, but no difference in inpatient spending or utilization.
What they didn’t look at was whether spending continued over time, or whether that additional expense was well spent, say, for preventive care.
Back to our model. In addition to the percentage of employed physicians, we measure five other dimensions to arrive at a composite DVI score:
- Quality of vertical integration: The degree to which the health system owns or has high-performing networks of health care delivery channels, such as physician groups, home health agencies and ambulatory surgery centers
- Technology integration: How integrated the system (hospitals, physicians and other service lines) is on a single EHR platform
- Payer experience: Whether the system has a health plan, how long it has had the health plan and how many lives are under management
- APM revenue: The estimated percentage of revenue tied to alternative payment models
- APM experience: The degree of sophistication with ACOs, bundles and other alternative payment models
To see what this model looks like, below you’ll see a side-by-side comparison of Dignity Health and Partners HealthCare.
The bottom line? We can’t say whether the trend is a good thing or a bad one, from the physician’s perspective or for the consumer. It’s a notable trend that’s likely to continue for the foreseeable future.
What else you need to know
Arkansas lawmakers are the first to pass a bill to regulate PBMs, reports the Arkansas Times. Signed into law on March 15 by Gov. Asa Hutchinson, the measure gives the state’s insurance commissioner the power to regulate the business practices of any PBM operating in Arkansas, including the authority to ensure that pharmacies are reimbursed sufficiently. More here.
Seven Next Generation ACOs have left the program for 2018, including: The Accountable Care Coalition of Chesapeake, Allina Health, Fairview Health Services, KentuckyOne Health, Lifeprint ACO, MemorialCare and Sharp HealthCare. Four of the seven withdrew because of changes that CMS made to the model—particularly the agency’s decision to lower the average risk score for 2017 by 4.82 percent, Modern Healthcare reported. Today, 51 ACOs remain in the program.
The Health Care Innovation Caucus in the U.S. House of Representatives was announced Thursday, and includes Reps. Mike Kelly (R-Pa.), Ron Kind (D-Wis.), Markwayne Mullin (R-Okla.) and Dr. Ami Bera (D-Calif.). Their focus is “to explore and advance successful, innovative payment models as well as the technologies needed to support these models.” More here.
Antibiotic-resistant infections remain a public health concern, but new research quantifies just how much it’s costing us. Using the Medicare Expenditure Panel Survey, researchers report that antibiotic resistance adds $1,383 to the cost of treating a patient with a bacterial infection. That amounts to $2.2 billion annually in health care costs. More here (subscription to Health Affairs required).
Aetna and Sutter Health have hired former Valence CEO Steve Wigginton to lead the joint venture they announced last year. The jointly owned health care company currently offers employers with employees in Northern California self-insured commercial products with effective dates as early as April 1, 2018. More here.
HCA said it has acquired Mission Health, a six-hospital health system based in Asheville, N.C. The deal marks the hospital chain’s first foray into the state. Terms were not disclosed. More here.
What we’re listening to